The Melanoma Landscape: 2007 vs. 2017
Only two treatments for patients with advanced melanoma were available in 2007: a chemotherapy, which wasn’t very effective and Interleukin 2, an immunotherapy that can be effective in a small group of patients, but also carries several side effects. In short, the prognosis for Stage IV melanoma was dismal.
However, change was on the horizon.
Promising research and drug development were underway and ideas were plentiful. Researchers were finally gaining momentum with immunotherapies and targeted therapies, which held great promise as new treatments that worked by mechanisms entirely different than any drugs previously used to treat melanoma.
/ Dedicated melanoma researchers with great ideas existed, the funding to support them didn’t—until Debra and Leon Black founded the Melanoma Research Alliance./
Dr. Jonathan Simons1 and Dr. Suzanne Topalian2 recall a melanoma landscape stifled by meager research funding and fragmented efforts. Federal and biotech funding was modest and very little was available from the philanthropic community to support melanoma research. Research was occurring globally; however, there were no efforts to connect researchers and research institutions. Dedicated melanoma researchers with great ideas existed, significant funding to support them didn’t—until Debra and Leon Black founded the Melanoma Research Alliance.
Melanoma Landscape: 2007 and 2017
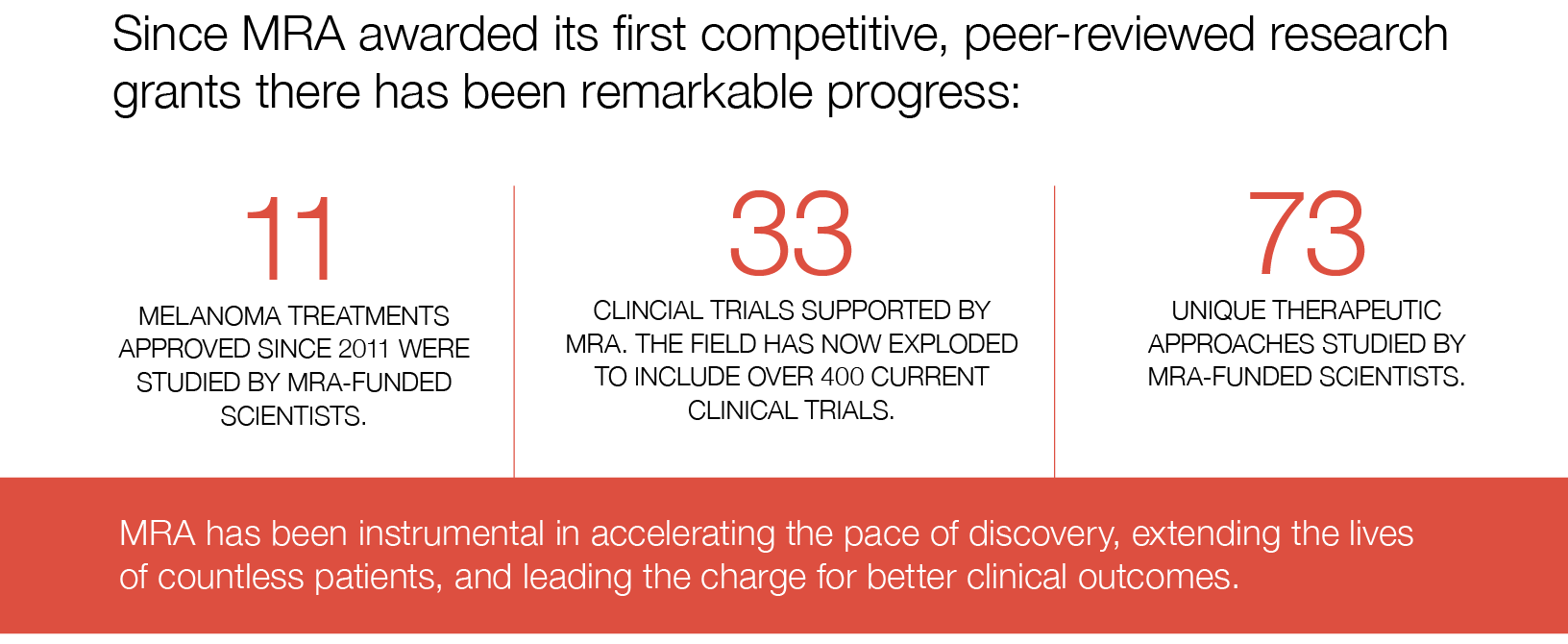
Comparing the melanoma landscapes are like comparing “color TV to black and white still photos,” says Dr. Simons. Melanoma was a specialized area in oncology garnering modest interest in 2007, recalls Dr. Topalian. In contrast, melanoma research is “center stage” today. With the infusion of research funds from MRA, groundbreaking advances have occurred in two major areas of oncology drug development: 1) targeted therapies and 2) immunotherapy.
These new advances have doubled the five-year survival rate for people with advanced late-stage metastatic melanoma, and new treatments and approaches on the horizon offer even greater hope.
Today, melanoma is the poster child for all of oncology. Lessons learned with checkpoint immunotherapies first approved for melanoma have now created new treatment options for lung cancer, bladder cancer, Hodgkin’s lymphoma, and head and neck cancer. In fact, immunotherapies are now being tested in over 30 cancers.
The Road to 2017
Dr. Simons and Dr. Topalian also attribute MRA’s transformative impact on the field to Debra Black’s personal experience with melanoma.
Debra’s unwavering courage, determination, and commitment to making a difference for patients with melanoma has positioned MRA as a true pathfinder for the next generation of therapies for treating and, ultimately, curing cancer.
Incubation under the auspices of the Milken Institute enabled MRA to benefit from learnings of several organizations.
MRA challenged the field to shift its focus to science with curative intent. It’s commitment to finding a cure for melanoma is reflected in its mission and exemplified in the research it funds.
Lastly, MRA’s philosophy of collaboration has been key to moving the field forward and is at the core of everything it does. It’s epitomized in the Team Science Award, a cornerstone of MRA’s scientific strategy.
MRA provides opportunities for researchers to interact with current collaborators as well as those with whom they wouldn’t have collaborated, under other circumstances. Historically, researchers in two major areas—immunotherapy and targeted molecular therapy—didn’t interact.
Today, that framework of commitment, curative intent, and collaboration persists. And, it’s been a defining characteristic of MRA as a shining beacon for so many patients who, without it, may not have hope.
The melanoma landscape has transformed significantly in the last 10 years, but continued support for melanoma research is critical.
While the melanoma treatment landscape has transformed, there is still much work to do. In 2007, when MRA was founded, just over 16% of late-stage metastatic melanoma patients expected to live five years after receiving their diagnosis; now, with new treatments, that figure has doubled. Yet the reality is that too many patients won’t benefit from even the latest advances. MRA is propelling progress on several fronts, such as testing new combinations of existing treatments and developing new targets that can be used for the development of entirely new classes of medication and therapies. This is MRA’s mission and we can’t achieve it without the dedication and support of our donors.
Together, with additional resources and continued focus, we will cure melanoma and transform oncology at large.
/ “I didn’t hear other organizations talking about a cure for cancer, especially not for melanoma. But, MRA approached its work differently. It understood that with the right research, we could cure melanoma and it wasn’t afraid to say so.” /
– Rusty Cline, melanoma survivor and advocate
1Simon, J. (Perosnal Interview) Jonathan Simon, M.D. is President and CEO of the Prostate Cancer Foundation and serves on the MRA Board of Directors.
2Topalian, S. (Personal Interview.) Suzanne Topalian, M.D. is a Professor of Surgery and Oncology, Johns Hopkins Medicine and a member of the MRA Board of Directors.