
Stage 3 melanoma, also known as regional melanoma, has spread to regional lymph nodes or nearby skin. Lymph nodes are an important part of the lymphatic system, which is a vast network of tissues and organs that helps rid the body of waste, toxins, and other unwanted materials. The lymphatic system also helps support the immune system by transporting infection-fighting white blood cells throughout the body.
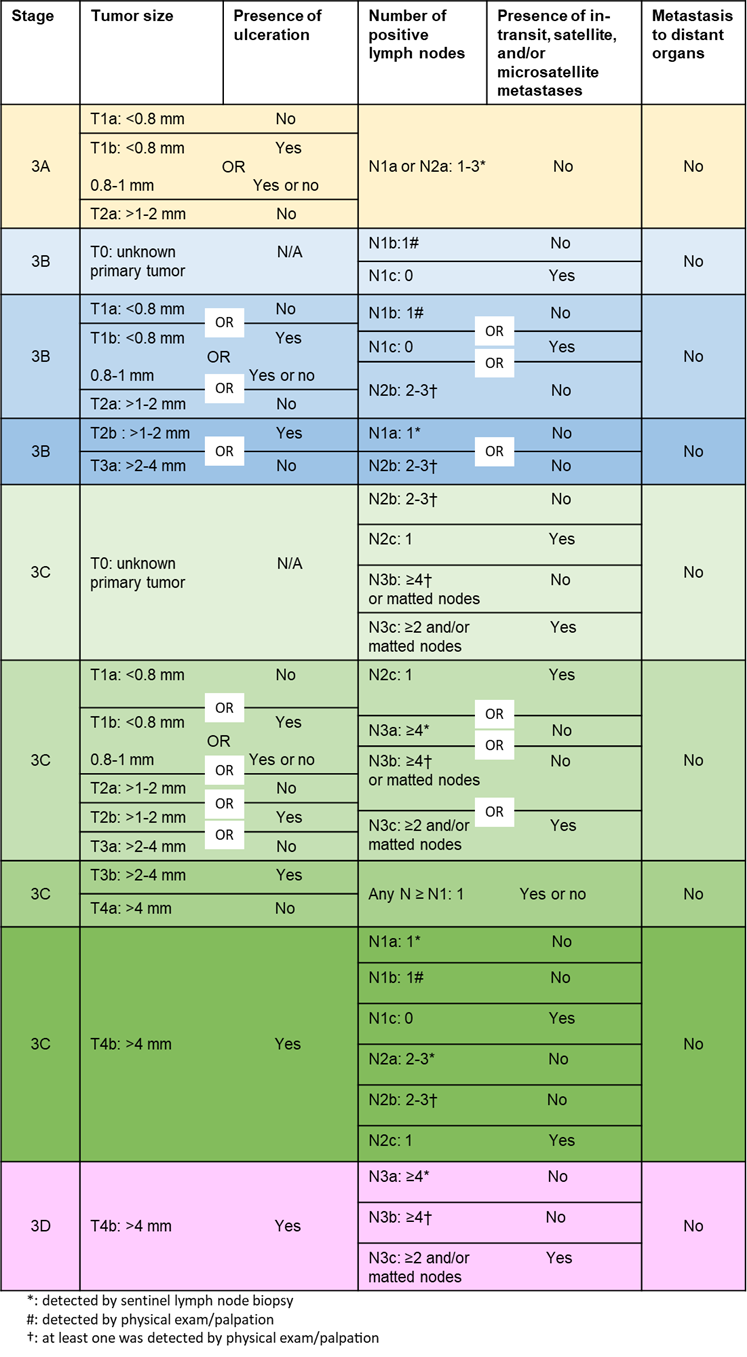
Stage 3 melanoma is divided into four subgroups based on ulceration of the primary tumor and the extent of growth into the lymph nodes and nearby skin.
In the below table:
Stage 3 melanoma treatment varies greatly depending on whether the melanoma is completely resectable. Melanoma that is resectable has been removed entirely with surgery. Melanoma that is unresectable cannot be removed completely through surgery alone. Learn more about melanoma treatment options.
Treatment for resectable stage 3 melanoma may first include treatment before surgery (called neoadjuvant). Neoadjuvant treatment may include immunotherapy (pembrolizumab or nivolumab and ipilimumab) or targeted therapy (if you have a BRAFV600 tumor biomarker) or both. Then, surgery with wide excision and lymph node dissection is often performed. Treatment after surgery (called adjuvant treatment) in patients where the melanoma is more likely to return may include systemic drugs such as immunotherapy or targeted drugs, radiation, or observation (depending on the risk of recurrence). Adjuvant therapy could be considered for melanoma detected in the sentinel lymph nodes (nearest lymph node to the tumor), especially for Stage 3B, 3C, or 3D melanomas.
Treatment options for unresectable stage 3 melanoma have expanded greatly in the last 10 years. Learn more about the different types of melanoma treatment options.
The preferred treatment for unresectable stage 3 melanoma is systemic therapy (immunotherapies and targeted therapies). Radiation therapy for symptomatic relief, oncolytic viral skin injections with T-VEC (Imlygic™), and best supportive care are also options.
Clinical trials offer patients access to treatment approaches that may be more beneficial than those currently approved by the U.S. Food and Drug Administration (FDA). In addition, clinical trials increase our understanding of melanoma and improve future treatment options for all patients. Given the very rapid development of new agents and combinations, patients are highly encouraged to talk to their physicians about the option of enrolling in a clinical trial for initial treatment and at the time of disease progression. Learn more about clinical trials.
With appropriate treatment, stage 3 melanoma is considered intermediate to high risk for recurrence or metastasis. With all melanoma, the earlier it is detected and treated, the better. Stage 3 melanomas are considered “regional”, meaning the cancer has spread past the area of skin where it started to nearby lymph nodes or other tissues. For Stage 3 melanoma, the melanoma-specific survival rate ranges from 93% to 32% 5 years after the initial melanoma diagnosis.
You should undergo a physical exam by your doctor every 3 to 6 months for the first 2 years, then every 3 to 12 months for the next 3 years, and then annually as needed. Imaging tests may be ordered every 3 to 12 months for 2 years and then every 6 to 12 months for the next 3 years to monitor for recurrence.
If you've been recently diagnosed with melanoma, you are not alone. The Melanoma > Exchange is a free online melanoma treatment and research-focused discussion group and support community.